The understanding of substance use disorder (SUD) or “addiction” as a chronic relapsing brain disease has improved over many decades and continues to evolve with science of evidence-based treatment and directly learning from individuals in long-term recovery. We know SUDs are most often pediatric-onset diseases: 9 in 10 adults with SUDs began drinking, smoking or using other substances before the age of 18.1 Thanks to advances in brain imaging, we also know that the human brain is not fully developed until about age 25,2 making adolescents uniquely vulnerable to substance use.3-4 As the nation looks to improve public health and reduce the astounding toll of overdose deaths and addiction, now is the time for a renewed focus on primary prevention – and when early substance use is initiated, provide effective intervention.
New Context to Youth Prevention Messaging
Youth substance use prevention efforts are often focused on individual substances, specific settings (e.g., impaired driving), and even specific amounts (e.g., binge drinking). While specific prevention messages are useful, they lack the context of the common patterns of substance use reported by youth. Nationally representative data from the National Survey on Drug Use and Health show that for young people, all substance use (and non-use) is closely related: among youth aged 12-17, the use of any one substance – alcohol, cigarettes, or marijuana – significantly increases the likelihood of using the other two substances and other illicit drugs.5 Similarly, not using any one substance significantly reduces the likelihood of using any other substances.
Figure 1 compares youth aged 12-17 who reported no use of alcohol in the past month (on the left) to those who reported various levels of past month alcohol use (on the right). Compared to their peers who did not use any alcohol in the past month, those who reported some alcohol use in the past month were 5.8 times more likely to have used marijuana, 3.8 times more likely to have used cigarettes and 4.8 times more likely to have used other illicit drugs. Youth who reported binge drinking (i.e., consuming 5+ drinks in one sitting) or heavy alcohol use (i.e., binge drinking 5+ times in the past month) were even more likely to have used marijuana, cigarettes, and other drugs.
Figure 1. Past Month Alcohol Use is Associated with Higher Use of Other Drugs Among Youth Aged 12-17

Source: National Survey on Drug Use and Health; DuPont, R. L., Han, B., Shea, C. L., & Madras, B. K. (2018). Drug use among youth: national survey data support a common liability of all drug use. Preventive Medicine, 113, 68-73.
The correlation of use holds true for other substances as shown in Figures 2 and 3. These data provide evidence for a generalized risk of substance use. Rooted in the science of the vulnerable developing brain, the goal of youth prevention can be reframed as, One Choice: no use of any alcohol, nicotine, marijuana. or other drugs by youth under age 21 for reasons of health.
Figure 2. Past Month Marijuana Use is Associated with Higher Use of Other Drugs Among Youth Aged 12-17

Source: National Survey on Drug Use and Health; DuPont, R. L., Han, B., Shea, C. L., & Madras, B. K. (2018). Drug use among youth: national survey data support a common liability of all drug use. Preventive Medicine, 113, 68-73.
Figure 3. Past Month Cigarette Use is Associated with Higher Use of Other Drugs Among Youth Aged 12-17

Source: National Survey on Drug Use and Health; DuPont, R. L., Han, B., Shea, C. L., & Madras, B. K. (2018). Drug use among youth: national survey data support a common liability of all drug use. Preventive Medicine, 113, 68-73.
Is Making One Choice of No Use a Realistic Goal?
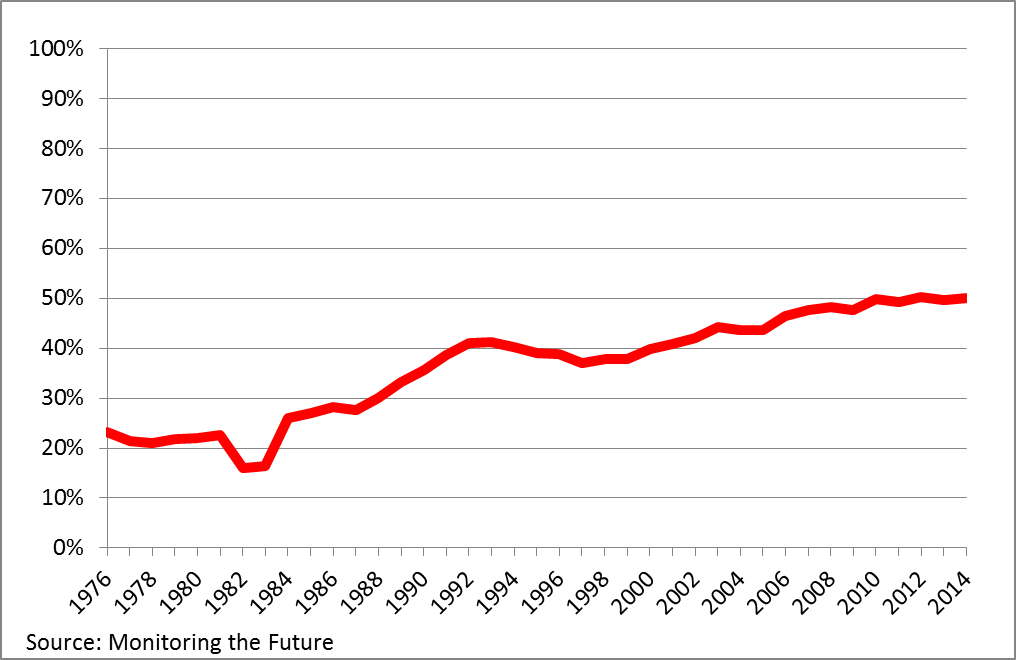
Parents and other adults may view adolescent substance use as inevitable or a rite of passage – but many American teens are already making One Choice today, and that number is growing.6 As shown in Figure 4, for decades, the percentage of American high school seniors who have not used any alcohol, cigarettes, marijuana, or other drugs in their lifetime has increased dramatically. The most recent Monitoring the Future data shows that in 2019, over 31% of high school seniors did not use any substances in their lifetime, and nearly 59% did not use any substances in the past month. These trends are also seen among 10th and 8th grade students.7
Figure 4. No Use of Alcohol, Cigarettes, Marijuana and Other Illicit Drugs by US High School Seniors, 1976-2019

Source: Monitoring the Future, 2019; Levy, S., Campbell, M. C., Shea, C. L., DuPont, C. M., & DuPont, R. L. (2020). Trends in substance nonuse by high school seniors: 1975–2018. Pediatrics, 146(6), e2020007187.
A New Health Standard for Youth
Just as the nation has embraced other health standards to support teen health – use a seat belt, wear a bicycle helmet, eat a healthy diet, avoid sugary drinks, and exercise regularly – together we can make no use of alcohol, nicotine, marijuana, or other drugs a new health standard for young people under age 21. This is not a reincarnation of the famous “Just Say No” campaign which focused on marijuana use. These data shows that alcohol, nicotine, and marijuana all dominate youth substance use and that the use of any of these three drugs is closely related to the use of all others.
Youth substance use is a health issue, not a moral issue. The One Choice goal is based on the science of the developing brain; highlights the long and strong youth-led trend in more young people refraining from substance use; follows legal age limits; and supports all other drug prevention efforts, including those that focus on single drugs and use in specific settings and specific amounts.
Teens are biologically driven to seek new and exciting behaviors which can put them at increased risk for substance use. Although use of alcohol, nicotine, marijuana, and other drugs is illegal for anyone under age 21 in the US, there are several factors that can make these substances more attractive to this age group including increased availability, normalization of use, and a decrease in perceived harm from use. As such, it is important to recognize the impact of Commercialized Recreational Pharmacology, defined as the super-stimulation of brain reward for profit.8 It is driven by the exploitation of people who use both legal and illegal substances and profits most off heaviest users. The US has a long and troubled history with the legal alcohol and tobacco industries related to youth, and now faces powerful, growing legal vaping and recreational cannabis (marijuana) industries that promote and profit from addiction to their products.
Take Action to Promote Adolescent Health and to Reduce the Toll of Future Addiction
Addiction is a preventable pediatric-onset disease; reducing the future prevalence of substance use disorders can begin with improving youth prevention. In this effort there are essential roles for parents, families, school and community leaders, health care providers and addiction professionals. What can caring adults do?
Articulate the One Choice goal as a health standard for young people. Talk early and often about expectations of no use before the age of 21 of any substances including alcohol, nicotine, and marijuana and its foundation of the science of the developing brain. Fit the One Choice goal into your family’s and community’s vision for youth health and wellness.
Identify substance use and intervene early. The American Academy of Pediatrics (AAP) provides guidelines for screening young patients for substance use, noting the importance of normalizing no use and of offering strong, supportive comments when no use is reported.9 When substance use is reported, brief interventions and, when needed, referral to treatment can make a positive difference in the health and wellness trajectory of a young person.
Amplify youth voices. Each year, more young Americans are making the decision to not use any alcohol, nicotine, marijuana, or other drugs. Give this growing group opportunities to share the reasons why they make One Choice and how that decision is working out for them.
Join the One Choice Community. The nation is searching for policies to reduce the burden of addiction on our nation’s families, communities, and health care, as well as how to save lives from opioid and other drug overdoses. We must begin this important work by promoting strong, clear public health prevention efforts based on the steady, sound, and clear support for no use of any alcohol, nicotine, marijuana, or other drugs for youth under age 21 for reasons of health.
We invite you to learn more about One Choice and how prevention groups are integrating the message and supporting data into prevention initiatives at www.OneChoicePrevention.org.
Robert L. DuPont, MD, IBH President
Caroline DuPont, MD, IBH Vice President
Corinne Shea, MA, IBH Director of Programs and Communications

References:
1 The National Center on Addiction and Substance Abuse at Columbia University. (2011). Adolescent Substance Use: America’s #1 Public Health Problem. New York, NY: Author. Available: https://drugfree.org/reports/adolescent-substance-use-americas-1-public-health-problem/
2 Gogtay, N., Giedd, J. N., Lusk, L., Hayashi, K. M., Greenstein, K., Vaituzis, A. C., Nugent III, T. F., Herman, D. H., Clasen, L. S., Toga, A. W., Rapoport, J. L., & Thompson, P. M. (2014). Dynamic mapping of human cortical development during childhood through early adulthood. PNAS, 101(21), 8174-8179. https://www.pnas.org/content/101/21/8174.full
3 DuPont, R. L. & Lieberman, J. A. (2014, May 9). Young brains on drugs [Editorial]. Science, 344(6184), 557. https://doi.org/10.1126/science.1254989
4 Volkow, N. D., Han, B., Einstein, E. B., & Compton, W. M. (2021). Prevalence of substance use disorders by time since first substance use among young people in the US. JAMA Pediatrics. https://doi.org/10.1001/jamapediatrics.2020.6981
5 DuPont, R. L., Han, B., Shea, C. L., & Madras, B. K. (2018). Drug use among youth: national survey data support a common liability of all drug use. Preventive Medicine, 113, 68-73. https://doi.org/10.1016/j.ypmed.2018.05.015
6 Levy, S., Campbell, M. C., Shea, C. L., DuPont, C. M., & DuPont, R. L. (2020). Trends in substance nonuse by high school seniors: 1975–2018. Pediatrics, 146(6), e2020007187. https://doi.org/10.1542/peds.2020-007187
7 Levy, S., Campbell, M. C., Shea, C. L., & DuPont, R. L. (2018). Trends in abstaining from substance use in adolescents: 1975-2014. Pediatrics, 142(2), e20173498. https://doi.org/10.1542/peds.2017-3498
8 DuPont, R. L., & Levy, S. (2020). The nation’s drug problem is commercial recreational pharmacology [From the Field]. Alcoholism & Drug Abuse Weekly, 32(35), 3-7. https://doi.org/10.1002/adaw.32827
9 Levy, S. J., Williams, J. F., & Committee on Substance Use and Prevention. (2016). Substance Use Screening, Brief Intervention, and Referral to Treatment. Pediatrics, 138(1), e20161211. https://doi.org/10.1542/peds.2016-1211